Tumours of the Mouth
This video was delivered to the Skin Cancer College Meeting at the Marriot in Surfers Paradise in March 2014.Tumours in the mouth are uncommon. The commonest is probably the simple viral wart or squamous papilloma. They tend to be rather filiform on the mucosal surfaces, particularly around the angle of the mouth and the vermillion border. Squamous cell carcinoma can commonly occur in the lips as can conditions such as lichen planus and lupus and paradoxically often a fungal infection of the lip where someone has applied strong topical steroid for a period of time. The lip is also a common site for lentigines particularly the labial melanotic macule seen often in young children after sunburn and the lentigines in the Putz Jaeger syndrome or in the Laugier - Hunziker syndrome.
Intraoral papules can also be seen in Darier's disease and in Crohn's disease, but these are both very uncommon. Leukoplakia on the surface of the lip and erythroplakia inside the mouth can sometimes be associated with squamous cell carcinoma, particularly the latter, and it should always be taken seriously. None the less one of the commonest causes of pigmentation inside the mouth is staining from an adjacent molar amalgam filling.
Let's start with some of these lesions.
Squamous papilloma is a benign proliferation of stratified squamous epithelium which gives rise to a wart like lesion. Some lesions may arise as a result of trauma but most are papilloma virus associated. Histopathologically there is proliferation of the stratified squamous epithelium with finger like projections with a fibrovascular core. Where the keratin layer is thickened, clinically the lesions are much whiter. Occasionally koilocytes are seen where virus alters the epithelial cells and they appear clear just under the stratum granulosum.
Common verruca vulgaris is very similar but histologically there is a more marked hyperkeratotic stratified squamous epithelium, again with finger like strands with a connective tissue core. The elongated ridges tend to converge towards the centre of the lesion giving a cupping picture and in the granular layer there may be clumped keratohyaline granules where clear cells called koilocytes are also seen. Sometimes eosinophilic intranuclear viral inclusions are seen in the cells in the granular layer in a verruca.


Sometimes the whole of the inside of the lip surface on the buccal surface is covered in flat topped papules and nodules and this is known as multifocal epithelial hyperplasia or Heck's disease. There is a viral induced proliferation of oral squamous epithelium, again due to the papilloma virus. There may be multiple areas seen and there is quite marked acanthosis of the oral epithelium.


This lesion looks like a wart but histologically there is an accumulation of lipid laden histiocytes hidden beneath the epithelium. Only rarely has papilloma virus been found and may represent a local reaction or immune response to local trauma or damage.
Is seen in the Putz Jaeger syndrome and the Laugier - Hunziker syndrome. Histologically there is an increased number of benign melanocytes along the basal area of the epidermis, clustered at the tips of the rete ridges and there is extra melanin amongst the basal keratinocytes as well. Sometimes some of the melanin has fallen into melanophages in the papillary dermis.
Pigmented macules in the mouth are usually labial melanotic macules, but rarely you can get oral melanocytic naevi, melanoacanthomas and melanomas. The vast majority are benign labial melanotic macules. These can occur at any age but are common in younger children. As well as on the external lips they can also be seen inside the mouth on the gingiva. Usually labial melanotic macules don't show the elongated rete ridges that you see in actinic lentigo. Note that there are a large number of systemic conditions that can give melanin pigmentation of the oral mucosa. We have mentioned Peutz Jaeger's and the Laugier - Hunziker syndromes. But you can also see it in dyskeratosis congenital and prominent oral pigmentation can occur in Addison's disease.
Drug such as Chlorquin have also been reported as causing oral pigmentation and rarely it can occur with Minocycline when it has been given in high doses.










Melanoacanthoma is a lesion we usually see on the back and regarded as a very dark seborrhoeic keratosis, but a similar lesion can occur around the oral mucosa with many melanocytes dispersed throughout the epithelium. Most commonly seen in dark skinned individuals and usually on the buccal mucosa. These lesions can rapidly increase in size and can be worrying of melanoma. In melanoacanthoma the dendritic melanocytes are scattered throughout the epithelial surface but you sometimes need special melanin stains to show this. They produce an excess of melanised keratinocytes contributing to the dark black colour.
Melanocytic naevi may occur on the vermillion surface of the lip or adjacent to it, but they can also occur inside the mouth and be both pigmented and non-pigmented. The junctional naevus typically has collections of benign looking naevus cells mainly at the tips of the rete ridges. Generally no treatment is required. Fortunately when a new pigmented lesion is raised in the inside of the mouth, it is thought to be a melanoma and this necessitates excision. I think it should always be done because oral melanoma, when it does occur, is associated with a poor prognosis. A blue naevus may sometimes be seen particularly on the hard palate.


Leukoplakia
Leukoplakia basically is a white patch or plaque that cannot be characterised clinically or pathologically as any other disease. This is the WHO definition, so it is a clinical definition. Histopathologically you may have just benign squamous hyperplasia giving rise to the leukoplakia, but if you have dysplasia or atypical cells then it may subsequently go on and develop an invasive squamous cell carcinoma.


Other conditions in the mouth that can cause white plaques include candida, lichen planus, chronic trauma to the cheek, friction, keratosis, nicotine stomatitis and leukedema and the white sponge naevus. Most cases of leukoplakia have to be biopsied.


Leukoplakia on the lips is typically due to ultra-violet radiation but also it is a feature of smoking and alcohol abuse. Large areas of homogenous or thick leukoplakia intra-orally are particularly a concern and should be biopsied in several areas. Verruciform leukoplakia can also occur and often preceeds the development of squamous cell carcinoma. It can be difficult to differentiate verrucous leukoplakia from an early verrucous carcinoma as they both have acanthosis with prominent papillary projections and blunted rete ridges.


Most cases of leukoplakia have no dysplasia on biopsy, probably only about 5 – 25% of cases will show dysplastic changes. These are regarded as enlarged nuclei, large and prominent nucleoli, increased nuclear dysplastic ratio, dark staining nuclei, clear polymorphic abnormally shaped nuclei and dyskeratosis, meaning premature keratinisation in epithelial cells. Obviously increased mitotic activity is worrisome as are abnormal mitotic figures. If dysplastic changes extend down the micro salivary glands in the floor of the mouth then this is also a worrying sign.
Oral Hairy Leukoplakia is a rare variant seen in HIV patients particularly along the sides of the tongue. It is a mixture of candida and EBV virus.
Oral Hairy Leukoplakia is a rare variant seen in HIV patients particularly along the sides of the tongue. It is a mixture of candida and EBV virus.
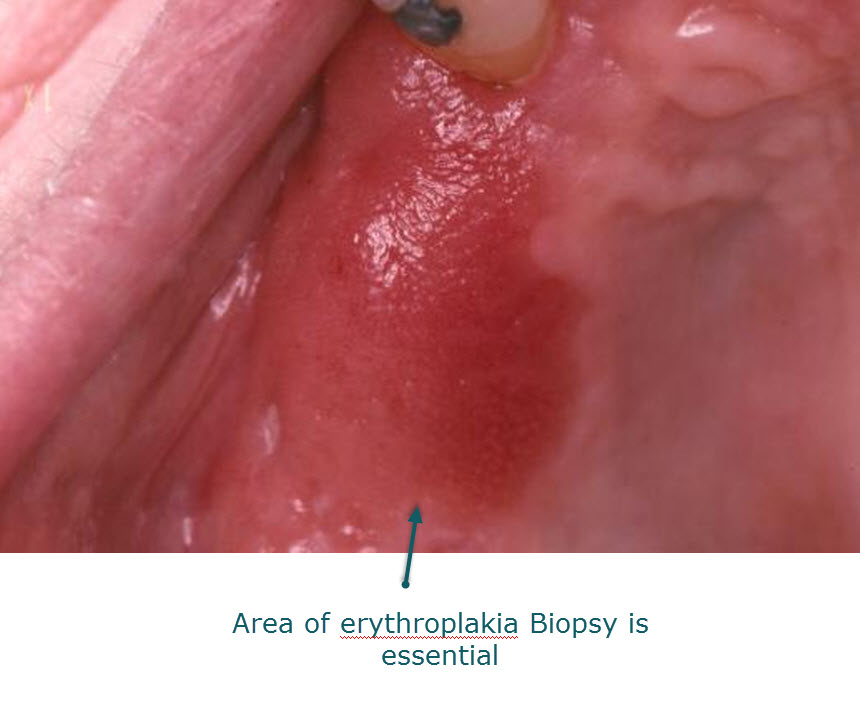
Oral erythroplakia is a more serious clinical finding. It is a red plaque on the inside of the mucosal surface. Virtually all cases will demonstrate significant epithelial dysplasia or carcinoma in situ. Some may even show squamous cell carcinoma. The causes are not really known but are thought to be the same as extensive leukoplakia with exposure to cigarette smoking, alcohol and chronic trauma. Erythroplakia and leukoplakia can commonly be found together. Generally the lesions are asymptomatic and have a smooth or velvety surface.

Nicotine stomatitis or smoker's palate used to be common when cigarette smoking and cigar smoking was common but this is not seen as often nowadays. It is a white keratotic change in the hard palate but it doesn't show dysplasia. However, if cigarettes are held with the lighted area inside the mouth then significant epithelial changes can occur.


Actinic cheilitis is obviously common on the vermillion border particularly the lower lip. It is due to chronic sun exposure over many years and the changes that are seen are very similar to those in actinic keratoses of the skin. Usually the stratified squamous epithelium is atrophic with excess keratin production. There may be epithelial dysplasia just in the lower two thirds of the epithelium with a lichenoid cellular infiltrate. Some elastotic changes may be seen in the connective tissue underlying the biopsy. Over time squamous cell carcinoma may develop in about 5% of cases of actinic cheilitis but is rare before 60 years of age.


Keratoacanthomas can be seen at the junction of the vermillion border and the lip and should be excised before they reach a size where they are going to cause significant deformity. They have similar features to the histology of keratoacanthomas elsewhere.


Squamous cell carcinoma of the oral cavity is unfortunately still increasing in incidence. It is seen particularly in aboriginal groups in Australia or in people who drink excessive alcohol and smoke excessively. In some parts of the world betel nut chewing is a relevant factor. Some cases of squamous cell carcinoma are due to oncogenic viruses and they may play a bigger part than we realise. SCC's on the inside of the mouth can be white or red and can easily bleed. Sometimes the lesions present as a hard nodule in the tongue. On the vermillion border of the lip typically they will present as a small ulcer that heals and then breaks down again and bleeds easily. People may confuse it with a healing cold sore but if it is occurring repeatedly or is taking a lot longer than two to three weeks to heal, then an SCC should be considered and a biopsy done.

Carcinoma of the tongue is often deep in the tongue and painless and just presents as an indurated mass. Rarely you will get an ulcer particularly on the lateral border. The other common site for squamous cell carcinomas is in the floor of the mouth under the tongue, so that when the mouth is being examined the tongue should always be raised and moved from side to side to check the under surface. Intraoral squamous cell carcinoma can spread to the local cervical or submental lymph glands and these should always be checked. Involvement of the parotid gland can also occur and is more serious stage.
Verrucous carcinoma of the mouth is a low grade malignancy, more wart like than cancer like, in that it doesn't metastasise but it has a blunt spreading edge to the rete ridges and dysplasia of the overlying epithelium. Generally this condition is seen in people over the age of 60.
Oral melanoma
This is a rare condition that is sometimes seen in only about 1 in a million or 1 in 2 million people annually. In studies it represents less than 1% of all melanomas. It may be more frequent in Japan and tends to present at a later stage and is usually painless. Most patients don't have a history of pre-existing pigmented lesion in their mouth. Any abnormal pigmented area in the mouth should be biopsied to exclude melanoma. In studies that have been done the prognosis is extremely poor, usually five year survival rate is somewhere around 15-20%. It is thought that this is due to early haematogenous spread of the tumour from the very vascular area in which it is found.


No comments:
Post a Comment
Note: Only a member of this blog may post a comment.